
Classifications
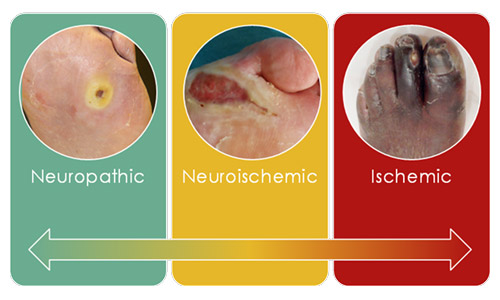
| FEATURE | NEUROPATHIC | NEUROISCHEMIC | ISCHEMIC |
|---|---|---|---|
| SENSATION | SENSORY LOSS | DEGREE OF SENSORY LOSS | PAIN |
| CALLUS/NECROSIS | PRESENT | MINIMAL CALLUS, PRONE TO NECROSIS | NECROSIS COMMON |
| WOUND BED | Pink and granulating, surrounded by callus | Poor granulation | Pale and sloughy with poor granulation |
| FOOT TEMPERATURE | Warm with bounding | Cool with absent pulses | Cool with absent pulses |
| OTHER | Dry skin and fissuring | Risk of infection | Delayed healing |
| TYPICAL LOCATION | Weight-bearing areas of the foot, such as metatarsal heads, the heel, and over the dorsum of clawed toes | Margins of the foot and toes | Nail edges and between the toes and lateral borders of the foot |
| PREVALENCE | 35% | 50% | 15% |
PERIPHERAL NEUROPATHIES
Sensory Neuropathy
Autonomic Neuropathy

Figure 3: Callus tissue in DFU Patients
Motor Neuropathy
Charcot Foot

Figure 5: Clinical Presentation of Charcot Foot
Peripheral Arterial Disease (PAD)
A New Chemical Entity
Diperoxochloric Acid (DPOCL)
Our office
Centaur Pharmaceuticals Pvt Ltd.
Mon - Fri: 9:00 - 18:00
Copyright © 2020 Centaur Pharmaceuticals Pvt Ltd.