
Assessment Tool
General assessment of the patient includes planning the physical/lab investigations for the patient including:
Diabetic Foot Examination
| SENSORY EXAMINATION | VASCULAR EXAMINATION | DEFORMITY | ULCER EXAMINATION |
|---|---|---|---|
| Vibratory perception: 128 Hz tuning fork or electronic tuning fork | Pedal pulses: dorsalis pedis, posterior tibial, perforating peroneal | Bunions, hammertoes, bone spurs, plantarflexed metatarsals, pes cavus foot type | Area, toe, metatarsal forefoot, lateral, medial |
| Achilles reflex | Erythema or cyanosis | Hallux limitus, Achilles/ gastro equinus, overpronation | Ischemic or neuropathic or mixed |
| Monofilament test 10 point touch [42] | Intermittent claudication score | Rocker bottom appearance | Small <10 cm, moderate 11–40 cm, severe >40 cm |
| Vibration perception threshold (VPT) | Temperature comparison between fee | Prior amputation | Cool with absent pulses |
| Temperature sensation | Dry skin and fissuring | Gait evaluation | Depth; probe test |
| Pain sensation | Vascular Doppler ultrasonography | Foot drop, atrophy, necrobiosis lipoidica diabeticorum | Healing or nonhealing (inflammatory granulating epithelialization) |
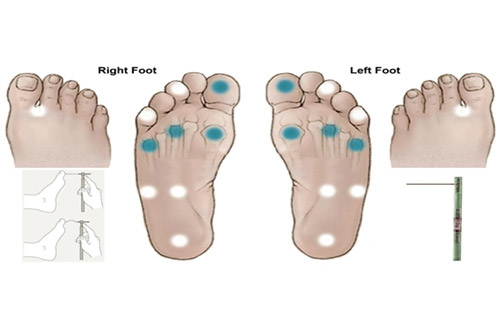
Figure 6: Demonstration of sensation test
Testing for Peripheral Arterial Disease
Parameters to examine in order to detect PAD:
Popliteal
Posterior tibial (PT)
Dorsalis pedis (DP)

Figure 7: Instrument to measure ankle-brachial pressure
Ankle-brachial pressure index
| Ischemia Grade | ABPI |
|---|---|
| 0 | ≥ 0.80 |
| 1 | 0.6-0.79 |
| 2 | 0.4-0.59 |
| 3 | ≤ 0.39 |
Measuring the Brachial Pressure
Measuring the Ankle Pressure
A New Chemical Entity
Diperoxochloric Acid (DPOCL)
Our office
Centaur Pharmaceuticals Pvt Ltd.
Mon - Fri: 9:00 - 18:00
Copyright © 2020 Centaur Pharmaceuticals Pvt Ltd.